
Sjogren’s Syndrome (SS) is a chronic autoimmune disorder that most commonly affects the glands that produce saliva and tears, leading to decreased production of saliva and tears. This causes the common symptoms of dry eyes and dry mouth.
The reported prevalence of primary SS varies widely, from 0.05% to 4.8% of the population and the frequency appears to increase with age. The diagnosis usually is made in midlife, but SS may occur at any age. The onset most often is insidious (slowly over time), and diagnosis may be delayed for many years. The disease is more common in females. SS may exist as a primary autoimmune disease, or as secondary to another underlying rheumatologic condition, such as rheumatoid arthritis or lupus.
The pathogenesis of SS remains unknown. It is thought that an as of yet unidentified environmental agent (like a virus) may trigger a cascade of events in genetically susceptible hosts, resulting in the development of SS. However, no specific inciting agent has been identified yet at this time. Due to the striking predominance of SS in women, it has been postulated that hormonal factors have a role in disease pathogenesis. Genetic factors play a role as well, and studies have shown that family members have an increased incidence of SS. Primary SS has been associated with an increased risk of cancer, particularly B-cell lymphoma.
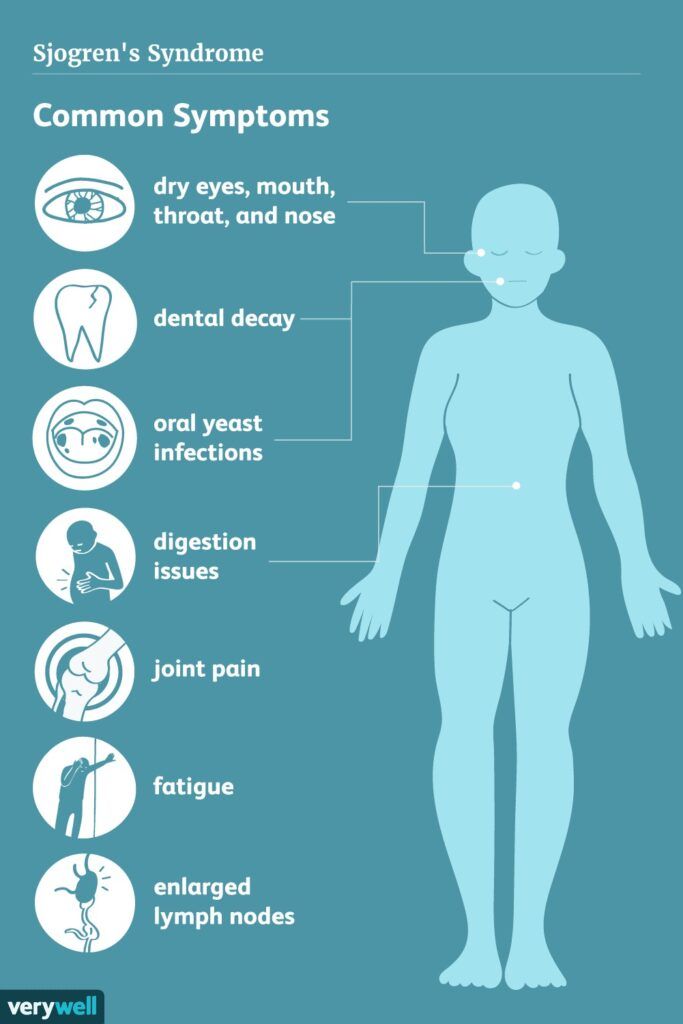
The main symptoms of Sjogren’s Syndrome are dry eyes and/or dry mouth. The dry mouth may lead to frequent cavities and dental infections. Other symptoms can include skin lesions, arthritis, respiratory symptoms, peripheral neuropathy, irritable bladder, and swollen lymph glands.