You’ve probably heard of Ozempic, Wegovy, Mounjaro, and other GLP-1 drugs. They are prescribed for type 2 diabetes, weight loss, and a growing list of health conditions. An estimated 1 in 8 adults in the US have already tried one, and that number keeps climbing.[1] Women between ages 50 and 64 are among the fastest-growing groups of users. Nearly one in three adults in this age group with diagnosed type 2 diabetes now take an injectable GLP-1.[2]
The Medicare GLP-1 Bridge, a new pilot program from Medicare Part D, started July 1, 2026, covering GLP-1 medications for $50 per month for qualifying patients.[3] Since Medicare previously didn’t cover GLP-1s for weight loss, this gives people over 65 new access, right as post-menopausal women, among those most at risk for bone loss, start taking a class of drugs that can weaken bones and speed up osteoporosis.
GLP-1s: What Are They?
GLP-1 drugs have been available by prescription in the US since 2005, originally to treat type 2 diabetes. It’s only in the last decade, starting with Ozempic, that newer versions have come along, curbing appetite and producing weight loss well beyond what earlier medications could do.
| Drug | Generic Name | Indication | Year Approved | Body Weight Loss |
| Ozempic | semaglutide | Type 2 Diabetes | 2017 | 5-7% |
| Wegovy | semaglutide | Obesity | 2021 | 10-15% |
| Mounjaro | tirzepatide | Type 2 Diabetes | 2022 | 7-14% |
| Zepbound | tirzepatide | Obesity | 2023 | 15-25% |
| Oral Wegovy | semaglutide | Obesity | 2025 | 13-14% |
| Foundayo | orforglipron | Obesity | 2026 | 11% |
Sources: FDA/manufacturer approval records [4]-[9]; weight-loss ranges from pivotal trials (SUSTAIN, STEP, SURPASS, ATTAIN, OASIS programs) [4]-[10].
These drugs work by mimicking a natural hormone in the body called GLP-1 (glucagon-like peptide-1), which helps regulate blood sugar and appetite. They slow down digestion and signal the brain that you’re full. The result is a combination that lowers blood sugar and drives significant weight loss. Thanks to how well they work, falling prices, wider availability, and now a pill option alongside the original injections, the use of GLP-1s has become more common across the US. They’re approved to treat type 2 diabetes and obesity. And they’re being studied for a growing list of related conditions, including:
- Cardiovascular Risk Reduction
- Chronic Kidney Disease
- Obstructive Sleep Apnea
- Fatty Liver Disease
- Many other conditions currently under study
How Do GLP-1s Affect Bone?
Right now, we don’t have a clear answer. The studies used to approve these drugs weren’t designed to look closely at bone health. But a growing body of evidence suggests GLP-1 treatment may weaken bones and raise the risk of osteoporosis.
The Research on Bone Loss from GLP-1s
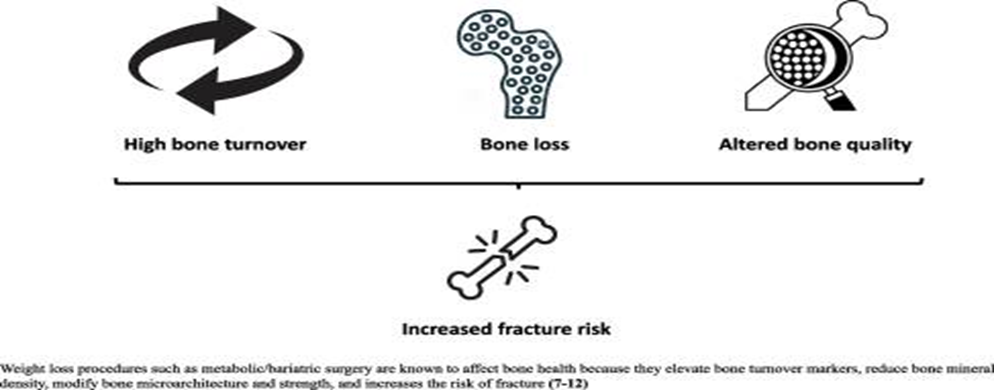
Significant weight loss disrupts the natural cycle of breaking down and rebuilding bone. Past a certain threshold, it ramps up osteoclasts, the cells that break down old bone, faster than the body can rebuild it, leaving bones less dense and raising the risk of osteoporosis and fractures. That threshold is roughly 7-10% of body weight, which all the most widely used GLP-1s cross within a year (see the table above).
For example, one 2024 study found that patients taking semaglutide (Ozempic, Wegovy) lost an average of 9.4% of their body weight over a year. They also lost bone density in the spine, and even more in the hip, compared to those on a placebo.[11] It’s still not clear whether the weight loss itself explains this, or whether something else about these drugs also affects bone directly. No study has settled that question yet.
The real-world picture on fractures is not clear at this time. SELECT, a major heart-health trial, followed over 17,000 people with existing heart disease taking semaglutide or a placebo for more than three years.[12] A safety analysis found nearly identical fracture rates in both groups, about 1.5% versus 1.7%, so no meaningfully higher risk showed up.[13] But SELECT mostly enrolled older men, a smaller portion were post-menopausal women who are at highest risk for bone loss. When an analysis of the postmenopausal women in the SELECT study was done it revealed that there was 5 times the rate of pelvic and hip fractures in this group. It also revealed that those over 75 years old had 4 times the rate of all fractures. These are concerning findings, and a comprehensive 2025 review agreed we still lack enough high-quality human data on long-term fracture risk cautioning that animal results don’t necessarily apply to people.[14] Targeted studies in the highest-risk patients are still needed specifically on postmenopausal women and the elderly who may be prescribed long term GLP1 therapy for obesity or diabetes.
A 2025 study also found that patients taking tirzepatide (Mounjaro, Zepbound) had a notably higher risk of osteoporosis and fractures than those taking other GLP-1s.[15] Since tirzepatide tends to produce more weight loss than other GLP-1s, this fits the broader pattern: weight loss appears to be the biggest single driver of bone loss in this drug class.
What Should Patients on GLP-1s Do to Protect Their Bones?
Nutrition: Strong bones depend on getting enough protein, calcium, and vitamin D. Because GLP-1s reduce appetite, it’s easy to fall short without realizing it. Ask your provider whether your diet or supplements need adjusting.
Exercise: Weight-bearing and resistance exercise protects bone, and matters even more for muscle, balance, and mobility. GLP-1s can cause muscle loss along with fat loss, which raises the risk of weakness, falls, and fractures. Everyone on a GLP-1 should have an exercise plan, especially those at higher risk of falls or fractures.
Evaluation and Treatment: Bone density testing is already recommended for people at risk of osteoporosis, including post-menopausal women and men over 70, and matters even more now that so many of them are taking GLP-1s. This quick, painless scan helps your doctor gauge fracture risk and decide whether a bone-protecting medication makes sense. Effective treatments exist, so in many cases this is a preventable problem.
GLP-1 drugs are transforming how we treat a wide range of health conditions. But we’re also learning that they may raise the risk of osteoporosis and bone fractures. Anyone taking, or prescribing, a GLP-1 should keep this in mind and take the steps above to protect bone health along the way.
By consulting with providers at Pacific Arthritis Care Center, patients in the Greater Los Angeles area who are taking GLP-1s, or would like to, can better understand and mitigate their potential risk for developing osteoporosis.
References
- Kirzinger A, et al. “1 in 8 Adults in the US Has Taken Ozempic or Another GLP-1 Drug.” KFF/CNN, May 10, 2024. https://www.cnn.com/2024/05/10/health/ozempic-glp-1-survey-kff
- Vahratian A, Warren A. “GLP-1 Injectable Use Among Adults With Diagnosed Diabetes: United States, 2024.” NCHS Data Brief No. 537, CDC, August 2025. https://www.cdc.gov/nchs/products/databriefs/db537.htm
- Centers for Medicare & Medicaid Services. “Medicare GLP-1 Bridge.” Accessed July 2026. https://www.cms.gov/medicare/coverage/prescription-drug-coverage/medicare-glp-1-bridge
- “Ozempic (semaglutide) FDA Approval History.” Drugs.com. First approved December 5, 2017. https://www.drugs.com/history/ozempic.html
- “Wegovy (semaglutide) FDA Approval History.” Drugs.com. First approved June 4, 2021. https://www.drugs.com/history/wegovy.html
- Eli Lilly and Company. “Tirzepatide Approved as Mounjaro by the FDA.” May 13, 2022. https://investor.lilly.com/news-releases/news-release-details/lillys-tirzepatide-shows-additional-211-weight-loss-after-12
- “Zepbound (tirzepatide) FDA Approval History.” Drugs.com. First approved November 8, 2023. https://www.drugs.com/history/zepbound.html
- Novo Nordisk. “FDA Approves Novo Nordisk’s Wegovy Pill, the First and Only Oral GLP-1 for Weight Loss in Adults.” December 22, 2025. https://www.novonordisk.com/content/nncorp/global/en/news-and-media/news-and-ir-materials/news-details.html?id=916472
- “Foundayo (orforglipron) FDA Approval History.” Drugs.com. First approved April 1, 2026. https://www.drugs.com/history/foundayo.html
- Novo Nordisk. “Weight Results, Ozempic (semaglutide) injection” (SUSTAIN FORTE trial); pooled SURPASS 1-5 body-weight results. https://www.novomedlink.com/diabetes/products/treatments/ozempic/efficacy-safety/ozempic-and-weight.html
- Hansen MS, Wölfel EM, Jeromdesella S, et al. “Once-weekly semaglutide versus placebo in adults with increased fracture risk: a randomised, double-blinded, two-centre, phase 2 trial.” eClinicalMedicine. 2024;72:102624. https://pmc.ncbi.nlm.nih.gov/articles/PMC11087719/
- Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. “Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes.” New England Journal of Medicine. 2023;389(24):2221-2232. https://doi.org/10.1056/NEJMoa2307563
- Kushner RF, Ryan DH, Deanfield J, et al. “Safety Profile of Semaglutide versus Placebo in the SELECT Study: A Randomized Controlled Trial.” Obesity. 2025;33(3):452-462. https://doi.org/10.1002/oby.24222
- Karam L, Mabilleau G, Paccou J. “Effects of Glucagon-Like Peptide-1 Receptor Agonists on Bone Health in People Living with Obesity.” Osteoporosis International. 2025;36(11):2115-2126. https://doi.org/10.1007/s00198-025-07664-1
- Hsu YH, Liang YC, Chan KC, et al. “Association of tirzepatide use with risk of osteoporosis compared with other GLP-1 receptor agonists: A retrospective cohort study using the TriNetX database.” Diabetes Research and Clinical Practice. 2025;230:112995. https://www.sciencedirect.com/science/article/abs/pii/S0168822725010101